Press release -
Phantom movements in augmented reality helps patients with chronic intractable phantom limb pain
Dr Max Ortiz Catalan at Chalmers University of Technology has developed a novel method of treating phantom limb pain using machine learning and augmented reality. This approach has been tested on over a dozen of amputees with chronic phantom limb pain who found no relief by other clinically available methods before. The new treatment reduced their pain by approximately 50 per cent, reports a clinical study published in The Lancet.
People who lose an arm or leg often experience phantom limb pain, as if the missing limb was still there. Phantom limb pain can become a serious chronic condition that significantly reduces the patients’ quality of life. It is still unclear why phantom limb pain and other phantom sensations occur.
Several medical and non-medical treatments have been proposed to alleviate phantom limb pain. Examples include mirror therapy, various types of medications, acupuncture, and implantable nerve stimulators. However, in many cases nothing helps. This was the situation for the 14 arm amputees who took part in the first clinical trial of a new treatment, invented by Chalmers researcher Max Ortiz Catalan, and further developed with his multidisciplinary team in the past years.
“We selected the most difficult cases from several clinics,” Dr Ortiz Catalan says. “We wanted to focus on patients with chronic phantom limb pain who had not responded to any treatments. Four of the patients were constantly medicated, and the others were not receiving any treatment at all because nothing they tried had helped them. They had been experiencing phantom limb pain for an average of 10 years.”
The patients were treated with the new method for 12 sessions. At the last session the intensity, frequency, and quality of pain had decreased by approximately 50 per cent. The intrusion of pain in sleep and activities of the daily living was also reduced by half. In addition, two of the four patients who were on analgesics were able to reduce their doses by 81 per cent and 33 per cent.
“The results are very encouraging, especially considering that these patients had tried up to four different treatment methods in the past with no satisfactory results,” Ortiz Catalan says. “In our study, we also saw that the pain continuously decreased all the way through to the last treatment. The fact that the pain reduction did not plateau suggests that further improvement could be achieved with more sessions.”
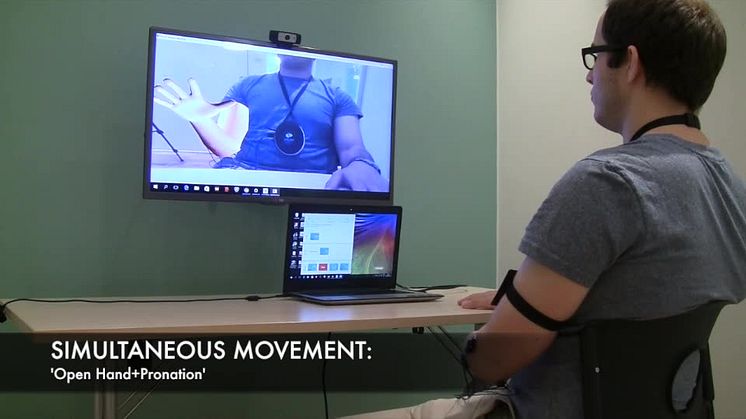
Ortiz Catalan calls the new method phantom motor execution. It consist of using muscle signals from the amputated limb to control augmented and virtual environments. Electric signals in the muscles are picked up by electrodes on the skin. Artificial intelligence algorithms translate the signals into movements of a virtual arm in real-time. The patients see themselves on a screen with the virtual arm in the place of the missing arm, and they can control it as they would control their biological arm.
Thus, the perceived phantom arm is brought to life by a virtual representation that the patient can see and control. This allows the patient to reactivate areas of the brain that were used to move the arm before it was amputated, which might be the reason that the phantom limb pain decrease. No other existing treatment for phantom limb pain generates such a reactivation of these areas of the brain with certainty. The research led by Ortiz Catalan not only creates new opportunities for clinical treatment, but it also contributes to our understanding of what happens in the brain when phantom pain occurs.
The clinical trial was conducted in collaboration with Sahlgrenska University Hospital in Gothenburg, Örebro University Hospital in Örebro, Bräcke Diakoni Rehabcenter Sfären in Stockholm, all in Sweden, and the University Rehabilitation Institute in Ljubljana, Slovenia.
“Our joint project was incredibly rewarding, and we now intend to go further with a larger controlled clinical trial,” Ortiz Catalan says. “The control group will be treated with one of the current treatment methods for phantom limb pain. This time we will also include leg amputees. More than 30 patients from several different countries will participate, and we will offer more treatment sessions to see if we can make the pain go away completely.”
The technology for phantom motor execution is available in two modalities – an open source research platform, and a clinically friendly version in the process of being commercialised by the Gothenburg-based company Integrum. The researchers believe that this technology could also be used for other patient groups who need to rehabilitate their movement capability, for example after a stroke, nerve damage or hand injury.
There are images at the bottom of this page.
Watch a video about how phantom motor execution works
More about: How the study was done
The patients were selected from three clinics in Sweden and one in Slovenia. They were treated with phantom motor execution twice a week for six weeks. They were asked to describe their pain levels before each treatment session and at follow-ups 1, 3 and 6 months after the end of treatment. To secure reliable pain measurements, several different ways of describing pain were employed, such as intensity, frequency, duration, quality, and the degree to which the pain affected sleep and daily activities.
More about: How phantom motor execution works
The treatment is based on a unique combination of several technologies Dr Max Ortiz Catalan and his team have developed:
- Conversion of muscle signals (myoelectric) into movements in a virtual arm. Some part of the arm must remain intact in order for signals to be detected, and the more arm muscles remain, the easier is to decode more movements.
- An augmented reality environment in which the patients see themselves on a screen with a virtual arm. Augmented reality is a combination of virtual reality and real information from the physical world. A fiducial marker on the stump allows the patient to move freely while the virtual arm follows along in the correct anatomical position.
- A computer game that the patients use to train the brain to send movement signals to the missing arm, in a fun, rewarding way.
No one knows exactly what causes phantom limb pain, but it is thought to be caused by changes in the brain that occur when a limb is lost. Phantom motor execution allows the patient to reactivate areas of the brain that were used to move the missing limb. Max Ortiz Catalan hypothesized that this can reset the changes in the brain that cause phantom limb pain. He also believes that a complementary mechanism for the pain relief is that the patients are learning to better use the muscles in their arm stump, which requires brain resources. The processing of pain signals also requires brain resources. So it may be that the new brain activity created by using the muscles in the stump “outcompetes” pain processing.
More about: Advantages of the method
Phantom motor execution has a several advantages over other methods to treat phantom limb pain:
- Creates an environment in which all parts fit together naturally. The patient’s desire to use the amputated limb activates the appropriate part of the brain and creates actual movement signals in the nerves and muscles of the stump, which leads to real-time visual feedback.
- Requires no surgical intervention and has no known side effects at present.
- Can be used even if both arms (or both legs) are amputated.
- Allows recreation of most movements that a natural arm (or leg) can make.
- Creates motivation using a computer game and precise measurements of the patient’s progress.
- Has a low cost compared to invasive treatment methods used today.
More about: The research
The paper Phantom motor execution facilitated by machine learning and augmented reality as treatment for phantom limb pain: a single group, clinical trial in patients with chronic intractable phantom limb pain was published online in the medical journal The Lancet on December 1.
Authors: Ortiz-Catalan M, Guðmundsdóttir RA, Kristoffersen MB, et al.
The study was a multidisciplinary collaboration between technical, medical, and industrial partners: Chalmers University of Technology (Gothenburg, Sweden), Sahlgrenska University Hospital (Gothenburg, Sweden), Örebro University Hospital (Örebro, Sweden), Bräcke Diakoni Rehabcenter Sfären (Stockholm, Sweden), University Rehabilitation Institute (Ljubljana, Slovenia), and Integrum AB (Mölndal, Sweden).
The study was funded by the Promobilia foundation, Vinnova, Jimmy Dahlstens Fond, Picosolve and Innovationskontor Väst.
Assistant Professor Max Ortiz Catalan recently founded the Biomechatronics and Neurorehabilitation Laboratory (Facebook and Twitter: @ChalmersBNL) at the Department of Signals and Systems, Chalmers University of Technology, where this work will continue.
For more information, please contact:
Max Ortiz Catalan, Department of Signals and Systems, Chalmers University of Technology, Sweden, +46 70 846 10 65, maxo@chalmers.se
Related links
Topics
- Medical research
Categories
- medical technology
- medicine
Chalmers University of Technology conducts research and offers
education in technology, science, shipping and architecture with a sustainable
future as its global vision. Chalmers is well-known for providing an effective
environment for innovation and has eight priority areas of international
significance – Built Environment, Energy, Information and Communication
Technology, Life Science Engineering, Materials Science, Nanoscience and Nanotechnology,
Production, and Transport.
Graphene Flagship, an FET Flagship initiative by the European
Commission, is coordinated by Chalmers. Situated in Gothenburg, Sweden,
Chalmers has 10,300 full-time students and 3,100 employees.